

The use of Neuro-Ultrasound to identify and treat nerve pathology

Advances in Musculoskeletal Ultrasound technology allows Physical Therapists and other healthcare providers to specifically identify nerve pathology and to therefore be able to potentially help patients more effectively. Ultrasound technology has been used in manual therapy professions for many years with the most frequent applications in the realms of both treatment and therapy, as ultrasound of a certain frequency can deliver therapeutic deep-heat into soft tissues. (van der Windt et al., 1999). Its usefulness in rehabilitation was established in the 1970s because of its ability to speed the healing process as a result of increasing blood flow in the treated area, decreasing pain, and during its application “massaging” muscles, tendons, and ligaments (Patil and Swami, 2017).
Other uses include delivery of medication to the subcutaneous tissues via the medium of ultrasound waves (Byl, 1995).
Advances in ultrasound technology (Harvey et al., 2002) have allowed health care providers to use high-frequency ultrasound to visualize muscle tissues, tendons, ligaments, nerves, bones and other structures (Whittaker et al., 2007). High-resolution ultrasound has also enabled healthcare providers to evaluate the integrity of neural tissues (Smith and Finnoff, 2009) In recent years neuro-sonography has been able to identify swellings of the nerve, proximal to the sites of compression, as well as changes in echo texture (Kara et al., 2012) See Fig. 1.
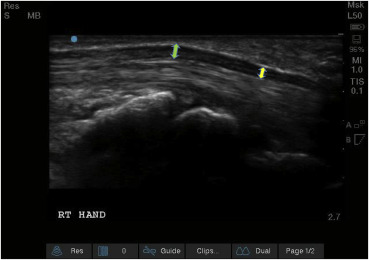
Notice the proximal swelling (left hand arrow) in comparison to the distal median nerve (right hand arrow) in long axis at the wrist. (With permission from Hands-On Seminars).
Normal peripheral nerves have a fascicular appearance where the individual nerve fibers and nerve fascicles have a hypoechoic (more black) echotexture, while the surrounding epineurial connective tissues have a hyperechoic (more white) echotexture. This is mentioned in the literature as a “starry night” or “honey-comb” appearance” (Jacobson, 2012) See Fig. 2.
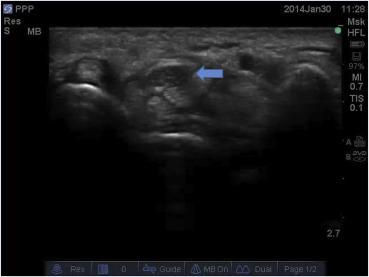
Median nerve in short axis at the site of the wrist. Notice the hypoechoic echotexture intermixed with the hyperechoic epineurium (arrow) (With permission from Hands-On Seminars).
Normal values have been established to measure the cross-sectional area of nerves as well as other ratios that help to distinguish pathological from normal tissue (Tagliafico and Martinoli, 2013) Swollen nerves tend to be more hypoechoic in echotexture, as they lose the honey-comb appearance which is characteristic of neural tissue in cross section, and produce cross-section measurements, greater than the normal values, due to nerve swelling (Jacobson, 2012, Tagliafico and Martinoli, 2013) See Fig. 3.
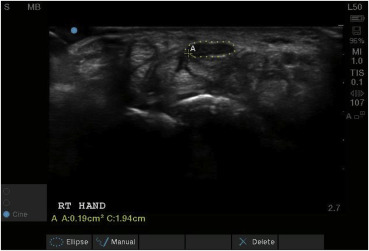
Cross section area of right median nerve measured at 0.19 cm2 which is moderately abnormal compared to normal value of <0.098 cm2 for the area measured.
Healthcare professionals may also evaluate neural pathology using electrodiagnostic evaluations (Armantrout et al., 2008). Electroneuromyography helps to identify the location of nerve pathology as well as the type of pathology (Kimura, 2017). Entrapment syndromes may cause displacement of the myelin sheath that surrounds the nerve axons, damaging the axon itself. Thus, nerve pathology can be classified as demyelinating, axonal, or both (Kimura, 2017, Kouyoumdjian et al., 2017).
A recent study published in the Journal of Ultrasound in Medicine (Moon et al., 2017) was able to investigate sonographic findings according to the pathophysiologic type, in patients with carpal tunnel syndrome. The researchers from Korea University School of Medicine retrospectively reviewed the records of 80 patients (148 hands) with carpal tunnel syndrome. They classified patients into three groups according to electrophysiologic findings: (1) conduction block and conduction delay; (2) axonal degeneration; and (3) mixed.
The study concluded that the cross-sectional area and wrist-to-forearm ratio were associated with the pathophysiologic type of carpal tunnel syndrome, with larger nerve swellings seen in patients with axonal degeneration compared with those with demyelinating lesions (Moon et al., 2017).
This is a breakthrough, as the results of the study enable healthcare providers who use Neuro-ultrasound, to use sonography, not only for localization of nerve lesions, but also for precise classification of the typeof nerve lesion. Once the location and type of lesion are identified, healthcare providers may use Neuro-Ultrasound to guide them in the performance of neural mobilization techniques (Ballestero-Pérez et al., 2017), to help restore normality.
Diagnostic Ultrasound technology can help the therapist not only to identify the nerve problem, but to also treat it with the highest possible accuracy and effectiveness (Kostopoulos and Rizopoulos, 2016).
In the USA most insurance companies reimburse Physical Therapists for the use of diagnostic musculoskeletal ultrasound, an approach that is rapidly gaining ground within that profession. Using musculoskeletal ultrasound sonography, healthcare professionals can visualize, in both static and dynamic capacity, several pathologies, such as rotator cuff tears, ligamentous laxities and tears, myofascial trigger points, nerve pathology and many others (Jacobson, 2012, Kostopoulos and Rizopoulos, 2016, Kumbhare et al., 2017) See Fig. 4.

Physical Therapist performing musculoskeletal ultrasound evaluation of the elbow joint.